

Nearly overnight, the coronavirus pandemic accomplished for digital health what decades of policy and reimbursement lobbying efforts could not; the sudden and widespread adoption of telehealth services for urgent and routine care. Although prior to COVID-19, there has been some evidence for increased satisfaction and efficiency of telehealth visits in primary care (1), it has recently been described in a summary of 58 systematic reviews, that evidence of clinical efficacy of telehealth visits has been lacking.(2) Nevertheless, despite the lack of robust clinical efficacy, the need for social distancing to limit spread of the coronavirus thrust the adoption of a digital health technology upon the healthcare system in a way never before seen. The resulting large-scale, natural experiment in telehealth is teaching us some early important lessons, but what lasting effects will telehealth have on the healthcare delivery system, and the ability for physicians to provide high quality care to patients remotely? And if you’ve liked telemedicine for remote visits with your doctor, will you get to keep it post-COVID?
Telehealth
Telehealth has been defined by the Centers for Medicare and Medicaid Services (CMS) as the exchange of medical information from one site to another through electronic communication to improve a patient’s health.(3) However, this definition has been broadened by some to span the use of information and telecommunications technologies in health care delivery for a specific patient involving a provider across distance or time.(2) Although some expansive definitions of telehealth cover both synchronous (audio and video enabled live visits), and asynchronous technologies (e.g. remote patient monitoring), the synchronous technologies such as video visits, have been boosted by the current pandemic in unprecedented ways.
Barriers: Reimbursement, Scalability, and Licensure
For years, telehealth has been touted as a promising approach to improving access to healthcare, and CMS has offered reimbursement for telehealth visits for Medicare beneficiaries in designated rural areas. But barriers to telehealth visit adoption have persisted, including disparities in access, technological limitations especially pertaining to limited broadband availability in underserved areas, reimbursement, medical licensure issues across state lines, and scalability.
Perhaps one of the largest barriers has been the complex reimbursement landscape. As CMS has offered reimbursement for an increasing variety of telehealth services, including televisit coverage for patients in designated rural areas, not only has legislation regarding telehealth reimbursement been conducted on a state by state basis,(4) but not all states have required telehealth service reimbursement to occur at the same rate as in-person services (i.e. incomplete parity laws). Furthermore, telehealth parity laws require private insurers to cover telehealth services, but not necessarily to cover the same spectrum and at the same reimbursement rates as Medicare. In effect, healthcare systems offering telehealth services can find themselves losing revenue relative to in-person visits, disincentivizing their use.
In its 2019 State of the States Report: Coverage and Reimbursement, the American Telemedicine Association noted that only 21 states and the District of Columbia had coverage parity policies in Medicaid services, and 36 + DC had parity policies for private payer coverage.(5) The net effect has been that only 11% of Americans, pre-COVID, had used telehealth for visits with their physicians.(5)
What COVID-19 did for Telehealth
According to an American Medical Association Study in 2019 predating COVID, 14% of physicians in the U.S. were providing synchronous telehealth visits in 2016, increasing to 28% by 2019.(5) To respond to the need to limit exposure of patients and healthcare providers to exposure, the federal government began relaxing previous restrictions on telehealth (Table 1). The effect, as reported in a McKinsey report was that in a matter of just a few weeks into the U.S. COVID-19 pandemic, 46% of Americans had used telehealth services,(6) a monthly growth rate of over 4,600% relative to the 3 years prior. Telehealth visits for Medicare seniors surged from a few thousand per week to just over 1.3 million.(7)
| Barrier | Coronavirus Pandemic Event | Changes to Barrier |
|---|---|---|
| Reimbursement | March 6, 2020 Emergency funding bill, Medicare 1135 Waiver | Temporary expansion of telehealth benefits to all Medicare beneficiaries, not just those in designated rural areas, as had previously been the case. |
| March 17, further expansion | Telehealth coverage for Medicare beneficiaries temporarily allowed for common office visits, mental health counseling, preventive health screenings. | |
| March 30, CMS further extends telehealth reimbursement | 85 additional telehealth services temporarily permitted. | |
| Licensure | March 13, 2020 Declaration of national emergency | Enabled the Department of Health and Human Services to waive federal licensing regulations, enabling out-of-state physicians to treat patients via telehealth. |
| Scalability | March 17, federal administration relaxes HIPAA penalties | Enables physicians to use platforms such as Facetime, Zoom, and Skype for to perform telehealth visits. |
| Apri 2, Federal Communications Commission provides $200M funding package | Equips healthcare providers with telehealth technology and implementation support. |
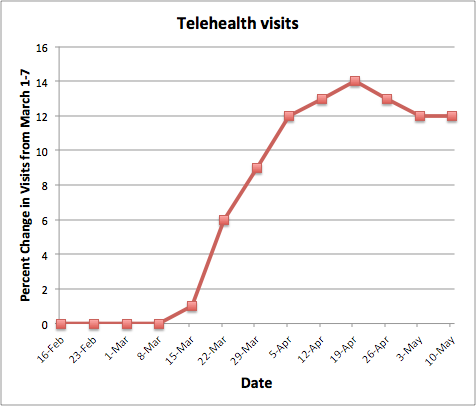
Figure 1. Telehealth service use pre and post COVID identifying percent change in visits . Data derived from (7)
Is This Telehealth’s Moment for Evidence?
What is the evidence that telehealth visits work? From a patient satisfaction perspective, the evidence is promising. In the McKinsey study(6), 74% of people who had used telehealth reported high satisfaction. But what are the clinical, cost, and safety outcomes, particularly if no vital signs are collected and if only a visual physical exam can be performed? In 2017, the National Quality Forum (NQF) published a report on a framework to measure telehealth quality and use of telehealth as a method of providing care. Domains studied for telehealth quality included: access to care, cost, cost effectiveness, and patient and clinician experiences. In 2019, the Agency for Healthcare Research and Quality (AHRQ) released a report on telehealth for acute and chronic care consultations which stated that telehealth results varied by setting and location but in general, telehealth consultations appeared to be non-inferior to controls. It also stated that the evidence for the benefits of telehealth was concentrated in certain use cases and specialty areas, with the strength of the evidence generally ranging from low to moderate. One of the areas in which televisits have rapidly expanded is within the Veterans Health Administration (VHA), the largest telehealth provider in the United States. Between February and March, the VA’s telehealth platform, VA Video Connect, saw the number of visits go from 41,000 to about 137,000 in March.(8)
In the current COVID-19 setting, telehealth is a great solution for patients with chronic conditions who need monitoring of medications and cannot postpone visits. Telehealth has also enabled virtual triage of patients and helped to keep patients safe in the midst of a pandemic.
In 2020, AHRQ evaluated the rapid adoption of telehealth during COVID-19 and provided meaningful insights based on its previous reports of research for both impact and effectiveness in telehealth. As stated in the white paper commentary, “the available evidence can help inform how we can apply telehealth wisely, while rapid adoption in a crisis provides opportunities to learn more, adding to the evidence base about telehealth.”(9) In order to understand how telehealth will emerge after the pandemic, it is important to consider how it can improve accessibility, clinical outcomes, and cost effectiveness for healthcare delivery.
Apart from costs, barriers to telehealth adoption are digital literacy gaps and access to technology for vulnerable populations. For example,1 in 7 households in Utah do not have an internet subscription, making these populations increasingly more vulnerable as they navigate a public health crisis without digital literacy skills and accessibility to telehealth. (10) To address this issue, Utah introduced House Bill 385 which proposed to create a Division of Digital Access and Opportunity. Such measures show the need to understand, educate and provide digital access in order to increase participation in telehealth and ensure that tools such as telehealth do not increase the digital divide for the most vulnerable members of our society while increasing access to immediate care.
What is in Store?
The McKinsey report estimated that post-COVID, approximately 20% of emergency department visits and 24% of healthcare office visits could be offloaded to telehealth, and that telehealth, recently a $3B industry, could balloon to a $250B industry.(6) But it is noteworthy that the federal policy changes of Table 1 are described as temporary. Does this mean that post-pandemic, reimbursement and licensure barriers for telehealth will be reinstated? Does this mean that if you’ve liked your telehealth visit, you won’t be able to continue to enjoy it? One eHealth tweet seemed to forebode this very possibility (Figure 2).

Figure 2. Shutting down telehealth post-COVID?
Some signals from federal lawmakers suggest that this natural experiment in telehealth was a wakeup call that barriers for telehealth need to remain down post-COVID. The effort to change has been an ongoing bipartisan issue, most recently leading 30 senators to appeal to the senate leadership (See letter here) to make many telehealth provisions of the 2017 CONNECT-for-health-Act permanent (11). In addition, G. K. Butterfield (NC-01) and Glenn Thompson (PA-15), have introduced the Helping Ensure Access to Local TeleHealth (HEALTH) act which looks to codify and make permanent telehealth funding to rural areas and community health centers (12). This bill offers a unique solution, specifically to health systems that struggle to scale telehealth due to inadequate reimbursement pre-COVID (13). Finally, representatives Diana DeGette (D-Colo) and Fred Upton (R-Mich) are working to unveil the next steps for 21st Century Cures Act 2.0 to strengthen telehealth. Upton stated, regarding the need for greater telehealth resources for safety net clinics, that “This is a technology that we need to have all across the country and not discriminate against areas just because they’re poor and rural.”(14) Sen. Brain Schatz (D-Hawaii) indicated that “Telehealth has rapidly transformed form a technocratic, wonky issue to an essential strategy for keeping people alive. We’re going to realize that all the changes we enacted ought to be permanent.” And Seema Varma of CMS said that “I just can’t imagine going back [to a time with less telehealth] because people recognize the value of this.”
Finally, the Senate Committee on Health, Education, Labor & Pensions started hearings on June 17th, called Telehealth: Lessons Learned from the COVID-19 Pandemic to discuss making permanent many of the changes that have been temporarily adopted during the coronavirus pandemic. Senator Lamar Alexander stated that our hospitals have been “forced to cram 10 years worth of telehealth visits into 3 months,” and that with the temporary changes in state and federal policies under the pandemic, we need to determine which changes should be kept, modified or reversed. Senator Alexander stated that of the 31 federal policy changes, most important in his mind are: 1. Reimbursement irrespective of patient location (originating site rule), 2. Medicare/Medicaid provider reimbursement for nearly twice as many telehealth services, and 3. Doctors allowed to conduct appointments during coronavirus using common video apps (relaxing federal privacy and security rules).
However, parity issues persist, making the prospects for telehealth a revenue-losing proposition for some healthcare systems, particularly those that operate on thin margins who are concerned about the high costs associated with maintaining telehealth platforms (up to hundreds of thousands of dollars annually), and reimbursement rates for telehealth visits that may be lower than for in-person visits. Others are concerned that permanent expansion of Medicare telehealth waivers and relaxation of privacy and security rules will offer increased opportunities for hackers seeking to gain access to protected health information. Ultimately, permanent expansion of some of the Medicare waivers will require Congressional approval. “It’s important for Congress to act this year.”
Widespread access to healthcare through video visits has come an incredible way in the last 3 months, but many barriers to making them permanent persist. So, don’t get too cozy with your new doctor on FaceTime. There are miles to go before this becomes a permanent part of practice, and the evidence that quality of care with these visits can be just as good as the standard of in-person care will be forthcoming in the months ahead.
NODE.Health Foundation is a 501(c)(3) non-profit organization dedicated to education, validation and dissemination of evidence based digital medicine. As the largest professional association in digital medicine, NODE.Health empowers societies, executives and NODES from health systems, payers, life sciences, venture capital, startups and the public sector involved in healthcare digital transformation. NODE.Health does not endorse any specific products or services.
NODE.Health is pleased to cross post this article giving examples of digital health solutions for telehealth. NODE.Health encourages its readers to be diligent with selecting such tools and understand the evidence. As more evidence comes out on the use of telehealth for COVID-19 and beyond, NODE.Health will keep its readers informed about the latest developments. Interested in learning more about the Network of Digital Evidence (NODE.Health)? Click here
References
- Karen Donelan, ScD, EdM; Esteban A. Barreto, MA; Sarah Sossong, MPH; Carie Michael, SM; Juan J. Estrada, MSc, MBA; Adam B. Cohen, MD; Janet Wozniak, MD; and Lee H. Schwamm, MD, Patient and Clinician Experiences With Telehealth for Patient Follow-up Care, Am J Manag Care. 2019;25(1):40-44 https://www.researchgate.net/profile/Esteban_Barreto/publication/330544973_Patient_and_Clinician_Experiences_With_Telehealth_for_Patient_Follow-up_Care/links/5c488050458515a4c73b127a/Patient-and-Clinician-Experiences-With-Telehealth-for-Patient-Follow-up-Care.pdf
- Totten A, Womack D, Eden K, McDonagh M, Grififn J, Grusing S, et al. Telehealth: Mapping the evidence for patient outcomes from systematic reviews. Rockville, MD: Agency for Healthcare Research and Quality (AHRQ), 2016. Report No. 26-EHC034-EF. https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/telehealth_technical-brief.pdf
- Fact sheet MEDICARE TELEMEDICINE HEALTH CARE PROVIDER FACT SHEET. (n.d.). Retrieved June 18, 2020, from https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet
- Harvey JB, Valenta S, Simpson K, Lyles M, McElligott J. Utilization of Outpatient Telehealth Services in Parity and Non-Parity States 2010-2015. Telemed J E Health. 2019;25(2):132‐136. doi:10.1089/tmj.2017.0265
- Ama-assn.org. 2020. [online] Available at: <https://www.ama-assn.org/system/files/2020-02/ama-digital-health-study.pdf> [Accessed 18 June 2020].
- Bestennyy O, Gilbert G, Harris A, Rost J. McKinsey and Company, May 29, 2020. Telehealth: A quarter-trillion-dollar Post-COVID-19 reality? https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality#
- Mehrotra A, Chernew M, Linetsky D, Hatch H, Culter D. The Impact of COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges. The Commonwealth Fund, May 19, 2020. www.commonwealthfund.org/publications/2020/apr/impact-covid-19-outpatient-visits
- Technology Solutions That Drive Government. 2020. VA Video Telehealth Program Keeps Up With Rapidly Expanding Demand. [online] Available at: <https://fedtechmagazine.com/article/2020/05/va-video-telehealth-program-keeps-rapidly-expanding-demand> [Accessed 18 June 2020].
- The Evidence Base For Telehealth: Reassurance In The Face Of Rapid Expansion During The COVID-19 Pandemic | Effective Health Care Program. [online] Available at: <https://effectivehealthcare.ahrq.gov/products/telehealth-expansion/white-paper> [Accessed 18 June 2020]
- Ravi, V., 2020. Vikram Ravi: Coronavirus Exposes Utah’S Digital Divide. [online] The Salt Lake Tribune. Available at: <https://www.sltrib.com/opinion/commentary/2020/03/21/vikram-ravi-coronavirus/> [Accessed 18 June 2020].
- Schatz.senate.gov. 2020. [online] Available at: <https://www.schatz.senate.gov/imo/media/doc/Letter%20to%20leadership_CONNECT%20for%20Health%20Act_06.12.20.pdf> [Accessed 18 June 2020].
- Representative G. K. Butterfield. 2020. Butterfield, Thompson Introduce The HEALTH Act. [online] Available at: <https://butterfield.house.gov/media-center/press-releases/butterfield-thompson-introduce-the-health-act> [Accessed 18 June 2020].
- Wu, G., 2020. Houston’s Health Care Systems Turn To Telemedicine To Meet Medical Needs. [online] HoustonChronicle.com. Available at: <https://www.houstonchronicle.com/business/article/Houston-s-health-care-systems-turn-to-15336883.php> [Accessed 18 June 2020].
- Degette.house.gov. 2020. [online] Available at: <https://degette.house.gov/sites/degette.house.gov/files/Cures%202.0%20Concept%20Paper_0.pdf> [Accessed 18 June 2020].


